 I've previously talked ranted about Google's web-browser Chrome and why you should master it to increase your productivity. Now here is a short tip I just picked up which will certainly save you time and mouse clicks while calculating your antibiotic dosing or critical care vital signs...
I've previously talked ranted about Google's web-browser Chrome and why you should master it to increase your productivity. Now here is a short tip I just picked up which will certainly save you time and mouse clicks while calculating your antibiotic dosing or critical care vital signs...Google search is so much more than just a brainless search motor, it has built in special functions providing for semantic search (in short, semantic in this aspect means more meaningful) results, just try for example looking up your flight number, "weather xxx" for an inine weather forecast, "define:xxx" for a quick explanation of a word and it's synonyms... you get the catch. There's also a calculator so that you can throw any numeric equation at it you wish to have crunched.
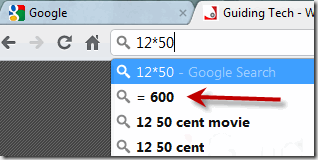
The real magic lies in Chrome's address bar, as I've previously mentioned it has some amazing features making it much more than just a browser. This is what I'm talking about:
Thanks Guidingtech for teaching me this trix (well worth reading too, you can never know too much about your browser, the heart and lungs of your computer)!
 With so many new websites appearing every week I find that the 'word by mouth' - personal reference from those you know - is the only way to "stumble upon" new webs today. Here is one gem I'd like to share with you.
With so many new websites appearing every week I find that the 'word by mouth' - personal reference from those you know - is the only way to "stumble upon" new webs today. Here is one gem I'd like to share with you.