And now I would give back and share with you those podcasts I enjoyed the most this year, hopefully inspiring you to try out the 'road lesser travelled' and waking up to the fantastic world of e-learning. Here they are, in no particular order:
- Having just had a tough case of bleeding aorta aneurysm with atrial fibrillation, Scott Weingart's rant about the crashing atrial fibrillation patient helped me understand better how to approach this 'shit has just hit the fan' scenario. This was how I discovered Weingart's amazing, almost aesthetic, collection of podcasts, bringing me EM wisdom in an unprecedented way.
- Scott's "Sympathetic Crashing Acute Pulmonary Edema" rant is also a ten bagger, I will never again be afraid of the dyspnoeic patient having razzles up to neck level.
- I have yet to dig through EM:Rap's wonderful collection of excellent EM lectures from all around the world but of those I've heard have already become all-time favorites. Especially I remember Michael Chansky's Diabetic emergencies as a total wow moment, the talk was so rich of valuable pearls I actually listened to it three times!*
- Stuart Swadron is one of my favorite EM ranters as the clinical pearls coming from his mouth are non-stop. Mel Herbert actually calls him "captain cortex" as he remembers the most petit symptoms and conditions. Earlier this year I listened to his discussion with Dr. Lopresti (who's seen more myxoedematous comas than any other physician!) about severe hypothyroidism in the EM; the ominous yet subtle presentations that you could easily miss in your ED. If you haven't already that is... In an hour's listening I learned more than my 3 month rotation to the endocrine clinic. In EM:Rap's june 2010 episode the same party discussed hyperthyroidism.*
- At Kos 2011, I had the fortune to enjoy Joe Lex's stunning talk about the assassinations of the american presidents, from the medical perspective. A lesser known fact to the world is that some of the deaths may actually have been early recordings of a medical malpractice as the patients (the presidents) were treated with utterly unsterile techniques. As Guiteau said himself in court: "The doctors killed Garfield, I just shot him". Even more stunning though is that these talks are free to listen to from freeemergencytalks.
- Definitely not the most educating EM podcast but absolutely the most entertaining one, what else would you expect from Mel Herbert? "Famous Deaths!" from Doctor's Unplugged and make sure you have plenty of floor space to ROFL!
- You know Rosen's textbook of Emergency medicine... well can you imagine this respected author and honored emergency physician telling you about the first years of emergency medicine, back in USA in the 1950s? Be prepared to hear one of the most interesting and even shocking EM talks you'll ever hear; Peter Rosen: Beginnings of Emergency Medicine. BTW Rosen's talk can also be viewed on All LA as a video-talk.
- ICU Rounds is a non-EM podcast site but hellya the overlapping of these fields is so extensive anyways, it's just like two sides of a slice of bread... (I already hear the footsteps of ICU trolls coming to my blog). A podcast about acute kidney failure had all of my attention this year and has taught me wise things about a scenario which is otherwise so boring to read about that the textbooks are soaked of drool from snoozing.
- Amal Mattu is an old favorite of mine and his talks were in 2010 my eye opener to the world of podcasts, as I discovered the freeemergencytalks collection. This year I listened to his great talk emergencies in the geriatric patient - a gentle reminder that the elderlies are not to be taken lightly in the ED.
- Finally, something to remind you that the world of podcasts is just half the story - there are also lots of excellent 'videocasts' out there; talks from the big conferences, academic lectures, grand rounds etc. They might not be a thriller for you working in an academic ED where emergency medicine has been alive for 50+ years but for me where we're almost in the startholes, without senior specialists with experience dripping of their clothes, having a video lecture with occasional academic shouts from the audience in the background has changed everything... I've seen a lot of good ones in the year and I can't easily say one is better than the other but the USC case presentations, escorted by Captain Cortex amongst others have had a great impact for my learning curve. Try for instance this excellent presentation of two mystery cases - just sit back and enjoy!**
That will be all. If you're new to the fascinating world of blogs, podcasts and vodcasts I have a not too long yet detailed introductory post for you to prepare for your first e-date. By the way, I would really like to see your highligths too, please feel free to jot whatever sits at the top of your heads here below in the comments!
With that said I wish you all a happy Christmas and let's hope I manage before 2011 is over to finish my post about Linux - aren't you curious to know how that can have anything to do with emergency medicine!
* I decided to use this as a shout-out for Mel Herbert's excellent EM:Rap, if you haven't heard of it before then read my lips: you are missing one of the greatest educational sources for emergency physicians, ever! EM:Rap is not free but you will not regret a single cent of your purchase. To prove my case I have uploaded the above mentioned podcasts for you to try out (with Mel's permission).
** The same goes for EM Core Content, also a Mel Herbert production. As you might have noticed, Mel Herbert is a very productive physician indeed and I seriously suggest you read my post about his wonderworks! Please notice the video quality is consciously reduced as this is only a introductory video!
** The same goes for EM Core Content, also a Mel Herbert production. As you might have noticed, Mel Herbert is a very productive physician indeed and I seriously suggest you read my post about his wonderworks! Please notice the video quality is consciously reduced as this is only a introductory video!
 I am sure there are other colleges out there, in dark corners - having exactly the same problem. So I decided to start an experiment to see if we can relief the frustration with modern crowdsourcing. Therefor I have started a Google Docs document, open for everyone to edit, with a few questions from our group to kickstart this project.
I am sure there are other colleges out there, in dark corners - having exactly the same problem. So I decided to start an experiment to see if we can relief the frustration with modern crowdsourcing. Therefor I have started a Google Docs document, open for everyone to edit, with a few questions from our group to kickstart this project.  Judging by Blogger statistics this post has had very many readers so I assume the idea must be something my colleges are interested in. As I had suspected the text based format is not the best one if this is to roll on, for example there is no way to "upvote" a the best answers and just pushing answered questions further down is no good way of archiving old questions.
Judging by Blogger statistics this post has had very many readers so I assume the idea must be something my colleges are interested in. As I had suspected the text based format is not the best one if this is to roll on, for example there is no way to "upvote" a the best answers and just pushing answered questions further down is no good way of archiving old questions. In september 2011 I was at the
In september 2011 I was at the 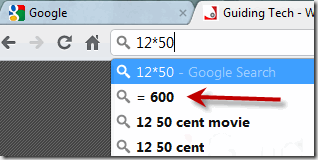 I've previously talked ranted about Google's web-browser Chrome
I've previously talked ranted about Google's web-browser Chrome  With so many new websites appearing every week I find that the 'word by mouth' - personal reference from those you know - is the only way to "stumble upon" new webs today. Here is one gem I'd like to share with you.
With so many new websites appearing every week I find that the 'word by mouth' - personal reference from those you know - is the only way to "stumble upon" new webs today. Here is one gem I'd like to share with you. If you're a newbie in the EM blogosphere, your first visit must be
If you're a newbie in the EM blogosphere, your first visit must be 

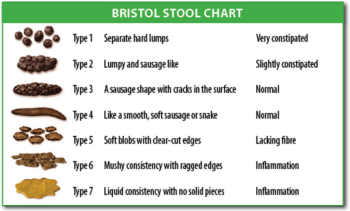
 Inferior MI and diseases of the upper gastrointestinal tract (gallbladder, stomach/esophagus especially) can present in very similar ways. Besides epigastric pain, patients commonly describe bloating and reflux-like symptoms due to vagal stimulation and gastric distension. Vagus stimulation explains why up to 40% of patients with inferior MI have sinus bradycardia (
Inferior MI and diseases of the upper gastrointestinal tract (gallbladder, stomach/esophagus especially) can present in very similar ways. Besides epigastric pain, patients commonly describe bloating and reflux-like symptoms due to vagal stimulation and gastric distension. Vagus stimulation explains why up to 40% of patients with inferior MI have sinus bradycardia ( We all remember those days when Microsoft Office was installed from some 25 or so diskettes and once setup up it was a permanent version not to be updated for a few years. With the Internet, updating became a little easier but you still had to manually download and install. Now that the web-browsers are becoming ever more powerful the software world is being taken over by
We all remember those days when Microsoft Office was installed from some 25 or so diskettes and once setup up it was a permanent version not to be updated for a few years. With the Internet, updating became a little easier but you still had to manually download and install. Now that the web-browsers are becoming ever more powerful the software world is being taken over by 
 is sometimes mentioned along with shock but there are other more common differential diagnoses such as decompression sickness, normal (cold) response in young children and a congenital variant (CMTC). All indicate instability in the vasculature (vasospasm/dilation). The patterns are unfortunately not uniformly defined as seen in the pictures on
is sometimes mentioned along with shock but there are other more common differential diagnoses such as decompression sickness, normal (cold) response in young children and a congenital variant (CMTC). All indicate instability in the vasculature (vasospasm/dilation). The patterns are unfortunately not uniformly defined as seen in the pictures on  is also connected with shock, as
is also connected with shock, as  That leaves us with only one option, email. Every doctor has an email and reads it on a daily basis or so. A server backup-ed, email based postlist system with functions to moderate content and members would be absolutely necessary. Members would want to have an option to login to change their profile and settings (receive immediately or digested content) and even go back in time and read older posts in the archive. Members should be able to see each others and even contact them individually. The system should still be closed for the public, that is - open for special registration/invitation only.
That leaves us with only one option, email. Every doctor has an email and reads it on a daily basis or so. A server backup-ed, email based postlist system with functions to moderate content and members would be absolutely necessary. Members would want to have an option to login to change their profile and settings (receive immediately or digested content) and even go back in time and read older posts in the archive. Members should be able to see each others and even contact them individually. The system should still be closed for the public, that is - open for special registration/invitation only.